 case report
case report Primary Cardiac Intimal Sarcoma with Extensive Left Atrial Involvement Treated with Cryoablation
Yu-Shan Huang1,2*, Fa-Po Chung1,2*, Tzu-Ting Kuo3,4#
1Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
2Institute of Clinical Medicine and Cardiovascular Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan
3Division of Cardiovascular Surgery, Department of Surgery, Taipei Veterans General Hospital, Taipei, Taiwan
4Depa rtment of Medicine, School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
*Both authors contributed equally to this work
#Corresponding author: Tzu-Ting Kuo, Division of Cardiovascular Surgery, Department of Surgery, Taipei Veterans General Hospital, No. 201, Sec. 2, Shih-Pai Road, Taipei, Taiwan
Received Date: 28 November, 2022
Accepted Date: 05 December, 2022
Published Date: 08 December, 2022
Citation: Huang YS, Chung FP, Kuo TT (2022) Primary Cardiac Intimal Sarcoma with Extensive Left Atrial Involvement Treated with Cryoablation. J Surg 7: 1654. DOI: https://doi.org/10.29011/2575-9760.001654
Abstract
A primary cardiac tumor is extremely rare. The majority of primary cardiac tumors are benign, and approximately one-quarter are malignant. The most common type of cardiac tumor is cardiac myxoma, which is usually located in the left atrium. Aside from the above, the majority of these malignant tumors are sarcomas, which can be distinguished by their different histologies. However, the differential diagnosis between benign myxomas and malignant sarcomas might be challenging in certain cases, and a high index of clinical suspicion and vimentin staining can be useful in making the diagnosis. In this case report, we present a young female who received an operation for a tumor of the left atrium that was initially diagnosed as a myxoma but later recurred as a myxofibrosarcoma. As a consequence of the immunoreactive results of MDM2 amplification, cardiac intimal sarcoma was finally diagnosed. It is notable that surgical removal of the primary tumor with extensive cryoablation of horizontal tumor spreading using a cryoballoon and cryoablation probe, which are initially designed for pulmonary vein isolation and Maze procedure, incorporated with postoperative radiotherapy, chemotherapy, and surgery to remove the costal bone metastasis effectively prevents the disease from relapsing and recurrences.
Keywords: Cardiac myxofibrosarcoma; Cardiac tumor; Cryoablation
Introduction
A primary cardiac tumor is very rare, and the majority of these (75%) are benign [1]. Among benign cardiac tumors, myxomas are the most common, whilst sarcomas comprise 95% of malignant primary cardiac tumors, which present with different histologies. Angiosarcomas, undifferentiated sarcomas, and undifferentiated pleomorphic sarcomas are the most prevalent types, with respective frequencies of 37%, 24%, and 11-24% [2]. At the time of diagnosis, primary cardiac sarcomas mainly affect adults with an average age of 41 years [3]. Of note, intimal sarcoma is the least reported primary malignant cardiac tumor, which occurs most commonly in the pulmonary veins and great vessels [4]. Complete surgical resection of primary cardiac sarcoma is the ideal treatment [2]. Unfortunately, this is not feasible in more than half of patients. Diagnostic delays, therapeutic difficulties, and a high degree of metastatic potential of cardiac sarcoma contribute to an extremely poor prognosis with a mean survival of just 3 months to 1 year [2]. Local recurrence and distant metastasis of cardiac sarcoma usually occur within one year and account for the poor prognosis [3]. In this report, we present a patient diagnosed with a primary cardiac intimal sarcoma, which was successfully treated by surgical excision, as well as extensive cryoablation of the primary lesion and local excision of bone metastases in conjunction with chemotherapy.
Case Report
A 26-year-old female with no known medical history presented to our hospital for consultation regarding a cardiac mass found during a transthoracic echocardiogram. The patient complained of fever, bloody sputum for several days, progressive exertional dyspnea, and paroxysmal nocturnal dyspnea for a few months. The results of the laboratory tests were insignificant. Chest CT revealed a large isoechoic mass in the left atrium (Figure 1), as well as shown in transthoracic echocardiography with tricuspid regurgitation, pulmonary hypertension, and right heart systolic dysfunction. Under cardiopulmonary bypass and the guidance of transesophageal echocardiography, tumor excision, mitral annuloplasty, and tricuspid annuloplasty were performed (Figure 2). Histological examination revealed predominantly a hypocellular myxoid tumor, composed of spindle-to-round cells within a myxoid matrix (Figure 3). We observed a focal area of increased cellularity with mild to moderate nuclear pleomorphism. Mitotic activity was rarely identified. A focal myxoid degeneration and infarct-type necrosis were observed. The tumor was reminiscent of cardiac myxoma due to its predominantly myxoid matrix.
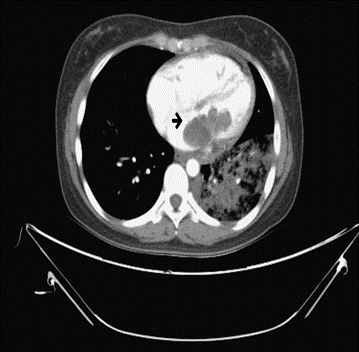
Figure 1: Post- contrast computed tomography: Revealing a lobulated low density in the left atrium, extending through mitral valve into left ventricle.

Figure 2: Intraoperative image: The large left atrium tumor and multiple round tumors adhesion to left atrium intraoperatively.
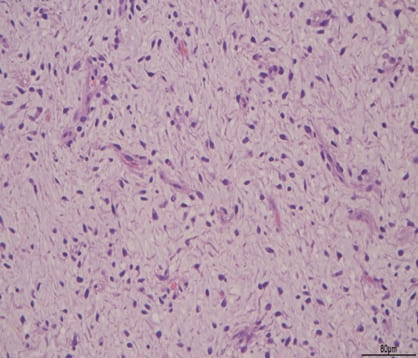
Figure 3: Pathology examination: Myxoid stroma and lepidic myxoma cells forming angiofomative complex are characterized by hematoxylin and eosin staining.
The patient was rehospitalized seven months later for tumor recurrence; a soft tissue nodule at the posterior wall of the left atrium was found in the follow-up CT scan (Figure 4). Repeat surgical resection was performed. There was a 5 mm x 5 mm nodule identified near the P2 mitral annulus. The tumor was removed extensively including excising the surrounding atrial wall with a 5mm radius, which was then repaired with a polytetrafluoroethylene patch. Focal endocardium thickening was noticed macroscopically, we performed two additional biopsies of the endocardium at the orifice of left atrial appendage and near P3 annulus respectively. The microscopic findings of all the specimens revealed a myxoid tumor which is similar to previous pathological findings. There was no evidence of CD34, SMA, or calretinin overexpression in the tumor cells. However, Ki-67 exhibited a higher level of staining in these atypical cells. The tumor resembled a cardiac myxoma from a morphological perspective. However, based on the relatively rapid growth of the tumor and the degree of nuclear atypia, the tumor was reclassified as a myxofibrosarcoma, grade II (Figure 5). Although the base margin of the tumors were free, it was assumed that the tumor had spread horizontally inside the left atrium without clear margin. As a result of the revised diagnosis of myxofibrosarcoma, another surgery was conducted. First, we did multiple random biopsies and sent for frozen section to define the area to treat. The intima was peeled using a scarpel as much as possible. Then cryoablation was performed all over the area, including inside left upper pulmonary vein, left lower pulmonary vein, and left atrial appendage, using a 28 mm second-generation cryoballoon (Medtronic, Minneapolis, MN), and a cryoICE cryoablation probe (AtriCure Inc, West Chester, OH) which were initially designed for pulmonary vein isolation and Maze procedure of patients with atrial fibrillation.

Figure 4: Computed tomography scan followed post surgery: Seven months after surgery, CT scans reveal a recurrent tumor (arrowhead) in the posterior wall of the left atrium.

Figure 5: Immunohistochemical study: The result demonstrates MDM2 overexpression.
Due to its unusual presentation, molecular analysis of the patient's original cardiac tumor resected at the first procedure revealed the tumor cells were immunoreactive to MDM2 and CDK4 gene amplification by Fluorescence in Situ Hybridization (FISH), which reflected a signature of intimal sarcoma. Furthermore, the presence of MDM2 and CDK4 gene amplification in the patient's cardiac tumor provided therapeutic implications in the future. Initially, the patient declined to undergo adjuvant chemotherapy. The post-operative radiation therapy was delivered over the surgical bed of recurrent tumor with a 5mm outer margin. A total of 6000cGy was delivered in 30 fractions using Simultaneous Integrated Boost Intensity-Modulated Radiotherapy (SIB-IMR). The chest CT follow-up at 3 months after the cryoablation therapy, as well as the serial chest CT every three months, revealed stationary cardiac conditions without local recurrence (Figure 6). However, 1 year after completing a course of radiotherapy, a chest CT showed a 4.2cm new expansile bone lesion at the right 10th rib, which was considered a metastasis. Thoracoscopic surgery was conducted with removal of the tumor at the right 10th rib and a wedge resection of the right lower lung. The resected sample from the rib demonstrated pleomorphic spindle to round cells in a myxoid matrix, consistent with metastatic cardiac sarcoma, while lung tissue and pleura were spared. In view of the presence of distant metastasis, an adjuvant chemotherapy regimen of Gemcitabine-Gemcitabine / Taxotere /Cisplatin plus everolimus (G-GTC+E) was administered over four cycles within two months. One month after completing chemotherapy, 5000cGy of radiation therapy in 20 fractions was delivered over the surgical bed of the right 10th rib. One year after treatment, the patient had neither local recurrences nor distant metastases of cardiac sarcoma.

Figure 6: A cartoon figure demonstrates the area of the left atrium receiving cryoablation (blue area).
Discussion
Primary Cardiac Tumor
The prevalence of primary cardiac tumors is extremely low [2]. The most common primary tumor in adults is cardiac myxoma. It is most common in females between the ages of 30 and 50, and over 75% of cardiac myxomas are located in the left atrium [6]. Cardiac myxomas usually have a myxoid stroma rich in elastin, collagen, and proteoglycan, with small fusiform or stellate cells and myxoma call, which have a round or oval nucleus and sparse eosinophilic cytoplasm. These cells frequently form rings, cords, and nests [7]. The majority of cardiac malignancies are sarcomas, which display a heterogeneous group of histologies. The histological subtypes of cardiac sarcomas include angiosarcoma, leiomyosarcoma, fibrosarcoma, rhabdomyosarcoma, synovial sarcoma, osteosarcoma, undifferentiated pleomorphic sarcoma, and intimal sarcoma [8]. Cardiac sarcomas can present in numerous ways and are well known for mimicking other conditions [2]. Patients may be asymptomatic until the condition reaches an advanced stage. The symptoms of cardiac sarcomas include dyspnea, orthopnea, paroxysmal nocturnal dyspnea, or lower extremity edema [9]. Patients with advanced stages of cancer can also present with symptoms of metastatic disease.
Cardiac intima sarcoma and immunohistochemical analysis Intimal sarcomas are poorly differentiated malignant tumors characterized by the formation of tightly packed, spindle-shaped cells with a fascicular growth pattern, and often with necrotic area. The intimal sarcoma, which is of mesenchymal origin, rarely affects the heart. However, once initial sarcomas occur in the heart, the left atrium and the mitral valve are commonly affected [1, 10]. A typical immunohistochemical analysis of these tumors demonstrates a positive reaction to MDM2, osteopontin, and vimentin. For ɑ-SMA, desmin, CD117, CD68, P53, and BCL-2, variable positivity is observed. In general, CD31, CD34, and Factor VIII are negative, but they may be positive in areas of angiosarcomatous differentiation [6]. The amplification of the MDM2 gene is a molecular marker of intimal sarcoma, which usually arises from large blood vessels of the systemic or pulmonary circulation [11]. Although it is extremely rare, primary cardiac intimal sarcomas are not recognized as distinct entities in the current WHO classification of cardiac tumors. Therefore, it is still debated whether to classify cardiac sarcoma with MDM2 gene amplification as intimal sarcoma. However, its importance lies in its potential therapeutic implication [12-14].
Treatment of Cardiac Intimal Sarcoma
A complete surgical resection with tumor-free margin is the primary treatment for cardiac sarcomas. However, 50% of patients are not suitable for this strategy because of the localization of the tumor and the difficulty to reconstruct after wide excision [3]. Intimal sarcomas are highly aggressive tumors with a mean survival ranging from 3 months to 1 year, although patients with cardiac intimal sarcoma who have survived for 11 years has been reported [15]. In addition, studies have shown that patients who have a complete tumor resection live twice as long as patients without the surgery [5,16]. Thus, early diagnosis and complete resection are of paramount importance in the management of intimal sarcomas. Moreover, local recurrences and metastasis are frequent and occur early, usually within one year [4]. Due to the rarity of cardiac intimal sarcoma, there is no definitive treatment guideline at present. Complete resection of the tumor remains the mainstay to cure primary cardiac intimal sarcoma.
However, clinical hurdles persist in removing extensive LA seeding, which renders complete resection impossible. Consequently, cryoablation of the surrounding tissue serves as a bailout strategy to prevent local recurrences. Ujihira et al. reported the application of cryoablation to treat cardiac myxofibrosarcoma with extensive involvement of the left atrium with excellent results, which was consistent with our results [17]. Cryotherapy has been established to treat cancers from heterogeneous origins. The extreme hypothermia produced by liquified argon results in ice crystal formation within tumor cells and lead to tumor necrosis. The cryoballoon and cryoICE cryoablation probe, were originally designed for pulmonary vein isolation in patients with atrial fibrillation, and can both produce profound transmural penetration of the lethal temperature [18,19].
Reviewing the photomicrograph of the sarcoma in our patient, the depth of tumor was limited to 2mm which can be easily engulfed by cryoablation. While cryoballoon provides better contact of the endocardial surface and large, homogeneous lesions, cryoICE cryoablation probe creates lesions deep into pulmonary vein and left atrial appendage and linear lesion to draw the contour of the treated zone. To the best of our knowledge, this is the first report to demonstrate the efficacy of cryoablation for a primary cardiac intimal sarcoma with left atrial spreading.
Aside from the above, radiation therapy and chemotherapy are also available as treatment options. As is recommended for soft tissue sarcomas, adjuvant therapy is typically administered to patients who have had a surgically removed cardiac intimal sarcoma [20]. Our patient declined chemotherapy and received only radiation therapy after her third surgery. Although she is free from local recurrence, she developed distant metastasis afterwards. Adjuvant chemotherapy has been shown to improve the time to local and distant recurrences as well as overall survival in two meta-analyses [21,22]. They may also confer survival benefits in patients with cardiac sarcomas as well [4]. When treating soft tissue sarcomas in adults, the principal regimens of chemotherapy are ifosfamide-epirubicin (or doxorubicin) and CyVADIC (cyclophosphamide, vincristine, doxorubicin, and dacarbazine). These patients may also benefit from gemcitabine-based chemotherapy (as a single agent or in combination with docetaxel) according to the favorable response to these drugs in some trials evaluating their role in soft tissue sarcomas [23,24]. A variety of treatment therapies, including those focusing on MDM2 oncogene overexpression, are currently under investigation [25]. The use of proton beam therapy can effectively spare uninvolved cardiac structures, which is why it was used in this case to improve long-term survival [6].
Conclusions
Primary intimal sarcomas of the heart are rare malignant tumors that have a poor prognosis. Their clinical and histological characteristics may mimic benign tumors, such as myxomas. The immunohistochemical analysis of specific markers can be helpful in making a differential diagnosis. It is imperative that the entire tumor should be surgically resected in order to ensure survival. When the atrial wall is extensively involved, complete resection may be challenging and cryoablation may be an option for the bailout. A multidisciplinary approach, which includes resection of isolated metastatic tumors, radiotherapy, and adjuvant chemotherapy, has been shown to prevent local and distant recurrences and prolong survival.
Reference
- Burke A, Tavora F (2016) The 2015 WHO Classification of Tumors of the Heart and Pericardium. J Thorac Oncol 11: 441-452.
- Butany J, Nair V, Naseemuddin A, Nair G. M, Catton C, et al. (2005) Cardiac tumours: diagnosis and management. Lancet Oncol 6: 219-228.
- Valecha G, Pau, D, Nalluri N, Liu Y, Mohammad F, et al. (2016) Primary Intimal Sarcoma of the Left Atrium: An Incidental Finding on Routine Echocardiography. Rare Tumors 8: 6389.
- Gupta A (2008) Primary cardiac sarcomas. Expert Rev Cardiovasc Ther 6: 1295-1297.
- Aboud A, Farha K, Hsieh WC, Brasch F, Ensminger S, et al. (2019) Prognostic Factors for Long-Term Survival after Surgical Resection of Primary Cardiac Sarcoma. Thorac Cardiovasc Surg 67: 665-671.
- Cho GJ, Kim HJ, Kang JS (2006) Primary cardiac sarcoma in pregnancy: a case report. J Korean Med Sci 21: 940-943.
- Di Vito A, Mignogna C, Donato G (2015) The mysterious pathways of cardiac myxomas: a review of histogenesis, pathogenesis and pathology. Histopathology 66: 321-332.
- Kuurstra EJ, Mullen JC, MacArthur RG (2014) Massive left atrial sarcoma presenting with severe congestive heart failure. Can J Cardiol 30: e1213-1255.
- Schiele S, Maurer SJ, Pujol Salvador C, Vitanova K, Weirich G, et al. (2019) Left Atrial Myxoma. Circ Cardiovasc Imaging 12: e008820.
- Ibrahim A, Luk A, Singhal P, Wan B, Zavodni A, et al. (2013) Primary intimal (spindle cell) sarcoma of the heart: a case report and review of the literature. Case Rep Med 2013.
- Neuville A, Collin F, Bruneval P, Parrens M, Thivolet F, et al. (2014) Intimal sarcoma is the most frequent primary cardiac sarcoma: clinicopathologic and molecular retrospective analysis of 100 primary cardiac sarcomas. Am J Surg Pathol 38: 461-469.
- Maleszewski JJ, Tavora F, Burke AP (2014) Do "intimal" sarcomas of the heart exist? Am J Surg Pathol 38: 1158-1159.
- Neuville A, Coindre JM (2014) Cardiac sarcoma with MDM2 amplification. Am J Surg Pathol 38: 1449.
- Sciot R (2021) MDM2 Amplified Sarcomas: A Literature Review. Diagnostics 11.
- Modi A, Lipnevicius A, Moorjani N, Haw M (2009) Prolonged survival with left atrial spindle cell sarcoma. Interact Cardiovasc Thorac Surg 8: 703-704.
- Burke AP, Cowan D, Virmani R (1992) Primary sarcomas of the heart. Cancer 69: 387-395.
- Ujihira K, Yamada A, Nishioka N, Iba Y, Maruyama R, et al. (2016) A case report of primary cardiac myxofibrosarcoma presenting with severe congestive heart failure. J Cardiothorac Surg 11: 95.
- Aryana A, Braegelmann KM, Lim HW, Ellenbogen KA (2020) Cryoballoon ablation dosing: From the bench to the bedside and back. Heart Rhythm 17: 1185-1192.
- Schill MR, Melby SJ, Speltz M, Breitbach M, Schuessler RB, et al. (2017) Evaluation of a Novel Cryoprobe for Atrial Ablation in a Chronic Ovine Model. Ann Thorac Surg 104: 1069-1073.
- Adjuvant chemotherapy for localised resectable soft-tissue sarcoma of adults: meta-analysis of individual data. Sarcoma Meta-analysis Collaboration 350: 1647-1654.
- Istl AC, Ruck JM, Morris CD, Levin AS, Meyer CF, et al. (2019) Call for improved design and reporting in soft tissue sarcoma studies: A systematic review and meta-analysis of chemotherapy and survival outcomes in resectable STS. J Surg Oncol 119: 824-835.
- Pervaiz N, Colterjohn N, Farrokhyar F, Tozer R, Figueredo A, et al. (2008) A systematic meta-analysis of randomized controlled trials of adjuvant chemotherapy for localized resectable soft-tissue sarcoma. Cancer 113: 573-581.
- Maki RG, Wathen JK, Patel SR, Priebat DA, Okuno SH, et al. (2007) Randomized phase II study of gemcitabine and docetaxel compared with gemcitabine alone in patients with metastatic soft tissue sarcomas: results of sarcoma alliance for research through collaboration study 002. J Clin Oncol 25: 2755-2763.
- Pautier P, Floquet A, Penel N, Piperno-Neumann S, Isambert N, et al. (2012) Randomized multicenter and stratified phase II study of gemcitabine alone versus gemcitabine and docetaxel in patients with metastatic or relapsed leiomyosarcomas: a Federation Nationale des Centres de Lutte Contre le Cancer (FNCLCC) French Sarcoma Group Study (TAXOGEM study). Oncologist 17: 1213-1220.
- Dewaele B, Floris G, Finalet-Ferreiro J, Fletcher CD, Coindre JM, et al. (2010) Coactivated platelet-derived growth factor receptor {alpha} and epidermal growth factor receptor are potential therapeutic targets in intimal sarcoma. Cancer Res 70: 7304-7314.