 research article
research article Rhinoplasty. A New Technique to Treat the Extremely Difficult Nasal Tip. Total Resection of the Alar Cartilages and Temporal Fascia. A 31-Year Experience
Salvador Rodríguez-Camps Devís
Division Chief of Aesthetic and Plastic Surgery, University Hospital Casa de Salud, Spain
Corresponding author: Salvador Rodríguez-Camps Devís, Division Chief of Aesthetic and Plastic Surgery, University Hospital Casa de Salud, Av. Manuel Candela, 46021 Valencia, Spain. Tel: +34963931515; +34963897700; +3434963897701; Email: cirugia-plastica@rodriguez-camps.com
Received Date: 26 March, 2018; Accepted Date: 27 April, 2018; Published Date: 07 May, 2018
1. Introduction
We present in this work a new technique which begins in 1987, 31-year experience till now. It was an impulse. Because of my reflexive character and perfectionism, it seemed contradictory and, yet, I sensed that this nasal tip, so badly arranged and anti-aesthetic after 3 operations, would only withstand a fourth operation which guaranteed certain success. So I thought that submitting the patient to a reconstruction of the whole cartilaginous nasal tip structure was not the best solution. Amputating and reconstructing seemed more complex and bloody than amputating and covering with some soft tissue. I chose temporal fascia as it is soft and not very extensible, and would provide the new tip more solidity. It came to my mind in a flash and I acted with all the consequences to help my patient. I did a follow-up and, years later, the result remained stable. However, as all the plastic surgery master’s treaties and publications warn us about the importance of conserving an alar cartilage band of no less than 3-5 mm on its caudal edge to avoid collapses, I thought that this process could wait before being repeated [1-8]. So gradually, I started performing more cases, and I saw that the result was no chance happening. I extended the indications and ventured with particularly difficult primary rhinoplasty cases involving extremely domed, flat and wide tips. The years went by and I continued improving and perfecting this process, which went against what was “technically correct”. Finally, we have classified our patients in 5 groups of cases which we name as: Type I, Type II, Type III, Type IV and Type V, depending on the resection-reconstruction process.
Since Roe and Joseph masterly established the basic concept of Modern Rhinoplasty in 1887 and 1904, upon which plastic surgeons still base ourselves today, research and contributions to this fascinating surgical technique have been constant, and each and every millimeter of the nasal pyramid has been studied and discussed from both the functional and aesthetic viewpoints. And all this always with the same maxim: “No excessive resection, and even less total resection, of alar cartilages given the risk of alar collapse”. Nonetheless for almost 31 years, we have studied, verified and finally demonstrated, with good results, that, yes, alar cartilages can be removed totally after correct diagnosis and suitable indication. A correct anatomical diagnosis of the tip and nasal base, and of the respiratory tract (septum, nasal turbinates and valves), and adequate indication, are always suitable in a nose whose tip is extremely difficult to correct with traditional techniques using cartilage grafts.
The purpose of this work is to present an extensive 31-year experience with a novel rhinoplasty technique of resection of alar cartilages and replacement with temporal fascia.
2. Keywords: Alar Cartilages Resection; Difficult Nasal Tip; Nasal
Tip; Nasal Base; Rhinoplasty; Temporal Fascia on Nasal Tip
1. Material and Methods
The indication for this new
technique is secondary rhinoplasty cases, for extremely difficult nasal tip
cases with broken or badly arranged cartilages, for traumatic rhinoplasty, and also for primary rhinoplasty situations in which the nasal tip is
excessively bulbous, disfigured, flat or wide. Where a “surgical tip” may
appear after the edema disappears, it is highly competitive with other
techniques based on complex cartilaginous structures with auricular grafts
[9]. We have 31 years’ experience (1987 - 2018) and more than 800 successful operations with fully satisfied patients. The refinement and beauty
of the nasal tip with a solid and equilateral base are the aim of this technique,
without historical prejudices and taboos; and we have
achieved this exactly [10-47].
In secondary and traumatic Rhinoplasty, for all type of nasal skin, suits this technique, always Rethi’s approach (Open Rhinoplasty), which is especially designed for it. Yet we are increasingly employing it in primary rhinoplasty when the solution for a cartilaginous dome proves difficult with other techniques. We are fully accelerating in this last case and have introduced some variation, as we will go on to explain. Mainly after cancer surgery on the nasal tip, we also have gained experience in nasal reconstruction [48].
1.1. The Resection
An equilateral and stable nasal base is our main objective. To fulfill this objective, we have classified resections into 5 types (although, in very special cases, it is convenient to make some little combinations between them).
This is indicated for noses that
are long-pointed, have a long columella,
and for large and elongated nostrils. Here we introduce some of our technical
resources, such as alar wedges, and resecting the crus medialis feet. Used
about 10% of the cases.
Many times, it is not necessary to use the temporal fascia for covering the crus medialis, because of the thickness of the skin. Used about 5% of the cases.
1.2. The Reconstruction
We place two stitches with 5-0 nylon, and conceal the knots, on top of the crus medialis to keep them firmly together. If the approach is complete, sometimes it is not necessary. A patch and/or a band of temporal fascia is placed covering the crus medialis.
1.3. The Temporal Fascia
In 1984, Dr. Guerrerosantos [49] introduced this procedure to
increase the dorsal unit of the nose and to fill the naso-frontal angle. We use
it for the tip to achieve a firm covering and a beautiful, smooth protection in
terms of both sight and touch by joining it as a single plane to the
fibroadipose covering to the skin. Baker and Courtiss [50] have demonstrated, through histopathologic
studies, that temporal fascia takes like a free graft in Rhinoplasty (1994) (Figure 11).
The seal extension will also depend on the thickness of the wings’ skin. We place 1 or 2-layered temporal fascia depending on requirements and the resection type, and we sometimes include muscle fibers to provide bulk.
In this way, the anatomy of the new nasal tip and the wings will outwardly to inwardly comprise the following single-body layers:
·
Superficial skin
·
Fibroadipose covering
·
External fibrous
lamina
·
Temporal fascia
·
Internal fibrous lamina
· Internal vestibular skin
1.4. The Postoperative Period
The postoperative period does not differ much with our technique from that of other techniques (if anything, recuperation is shorter). However, we have to maintain the vestibular cotton pads pushing the domes for 4-5 days. A plaster splint remains in place for 7 days, and a double layer of Steri-StripR is used for 7 additional days. The sensation of the nasal tip could be affected but only in the very first months and not in every patient.
4. Results
Judging from our patients’ degree of satisfaction, the results obtained since 1987 to date in 2018, range from very good to excellent, in one year following them (at 1 week, 2 weeks, 1 month, 3 months, 6 months and a year). Other nasal tip reconstruction techniques performed with complex cartilaginous structures did not provide us with the best results because a “surgical tip” emerged when the edema disappeared, with traces of barely admissible tips and edges.
We reconstruct the nasal tip using the cartilages we have available, and if they do not serve this purpose, we resect them directly. We very rarely resort to cartilaginous grafts since we adopted our technique. Personally, I reached the conclusion some time ago of NOT using cartilaginous grafts in the nasal tip, provided this is feasible, for ultimate problems of displacement, reabsorption, distortion and an unappealing presentation in terms of sight and touch.
Despite what I have stated herein,
I wish to express my maximum respect and admiration to all the Rhinoplasty
Masters from whom I have learnt. We have had no problems with the ever-feared
alar collapse, which is most certainly due to other factors such as an excessive resection of the triangular (lateral) cartilages, a vestibular valve lesion without correcting a significant deviation of the
septum during surgery, or hypertrophic turbinates which could contribute to or
even cause nasal respiratory failure with a uni or a
bilateral collapse. Regarding complications, there is nothing particular to
highlight in either aesthetic or functional terms. Only to outstand two nasal
infection cases due to the coincidence of sinusitis. We had neither revision at
all nor extrusion of temporal fascia. External valve collapse was not appreciated in any case.
5.Discussion
I realized that this technique was controversial, from the beginning, and that our Rhinoplasty Masters did no advice an excessive resection of alar cartilages, but preferred to maintain a cartilage band of a width of no less than 3-5 mm in the latero-caudal sense to avoid alar collapse. However, by following the steps of our technique and by maintaining its main objective (an equilateral, solid nasal base with a firm, yet soft nasal tip in terms of sight and touch, with no cartilaginous remains in view) I have verified and demonstrated that this may be avoided. Nonetheless, all this involves experience in rhinoplasty and a totally accurate technique. It proves a most useful technique, but to be used only in extremely difficult nasal tip cases.
6.Conclusion
My new technique has posed no problems when well indicated, diagnosed and performed, and has matured sufficiently over time in casuistry. Finally, the nasal tip becomes as firm and consistent, or more, than prior to surgery. Its five anatomical layers retract in a uniform fashion without distortions. To the touch, it is solid yet smooth and, aesthetically, it offers a beautiful result. Our colleagues should trust in the technique thanks to its results. I literally cite: … “The author must be congratulated for his work, and be honored and highly commended for the results obtained. This study is unique and it offers excellent results” … “Indeed, these results will convince many of us in practicing these aggressive resections” …
“The complete and permanent removal of what Mother Nature has designed requires the broadest experience, competence and an aesthetic feel by a Master Craftsman in a procedure that permits a minor error, or absolutely none. I therefore completely agree with the author that this procedure cannot be generally applied to all nasal tip operations, and that it is not suitable for enthusiastic beginners in surgery who lack both experience and aesthetic criteria” … “It is likely that the author has found temporal fascia an ideal substitute after totally resecting alar cartilages. (Dr. Neeta Patel, in her commentary on this technique in the Aesthetic Plastic Surgery Journal. January 2009).
Furthermore: “Dr. Rodríguez-Camps’ contribution makes this nasal tip technique most interesting for difficult cases” …“We are well aware that the nasal tip is one of the most difficult parts of Rhinoplasty, and that all of us have the technique that provides the best results available; but we also know that some rhinoplasty cases are very difficult to solve. Dr. Rodríguez-Camps’ technique of totally removing alar cartilages and then introducing temporal fascia is novel and interesting” … “Needless to say, the results obtained by Dr. Rodríguez-Camps are excellent and we are enthusiastic about using this nasal aesthetic technique” (Dr. Guerrerosantos in his commentary on the technique in Cirugía Plástica Iberolatinoamericana. Jan.-Feb.-March 2010).
We conclude that when it seemed
that everything had been described, and that the results depended only on our
hands, something new and fresh appears: “The Total Resection of the Alar
Cartilages and Temporal Fascia Technique”.
3.1.1. Type I (Figure 1,2)
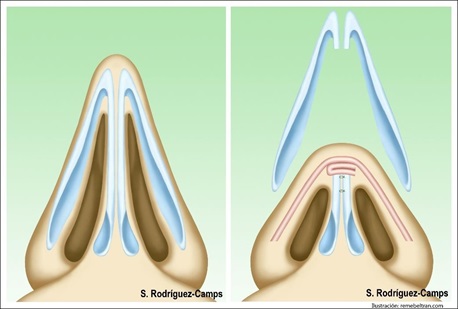
Figure 1: Illustration of the Type I.
Total Resection of the Alar Cartilages, including Domes and a portion of Crus
Medialis. Patch and ban
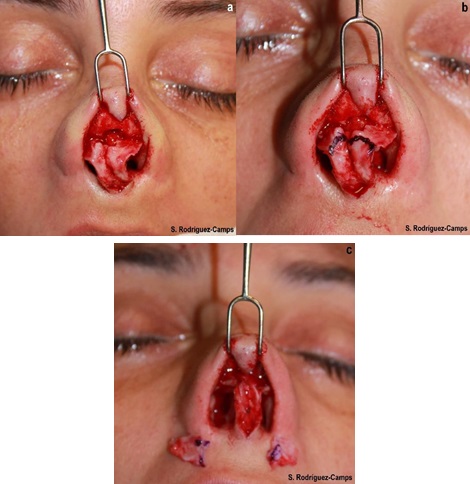
Figure 2: Type I.
Complete resection of alar cartilages, including domes and one trunk of the
crus medialis. Patch and Band of Temporal Fascia.
3.1.2.
Type II (Figure 3,4)
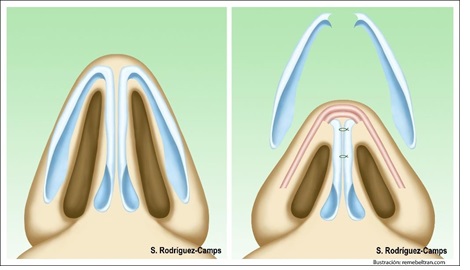
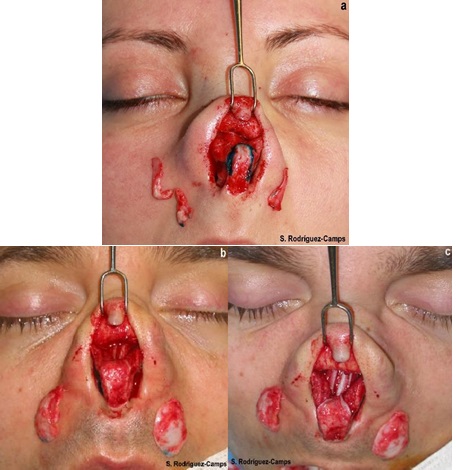
Figure 4: Type II. Complete resection of alar
cartilages, including domes. This is indicated for noses with a slightly
elongated nasal base. Patch and Band of Temporal Fascia. Used about 20% of the
cases.
3.1.3. Type III (Figure 5,6)
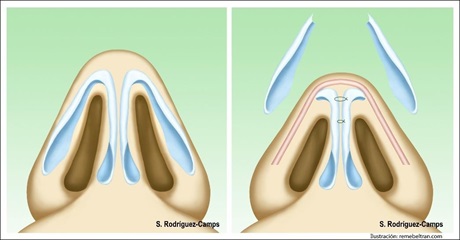
Figure 5: Illustration Type III. Total
Resection of the Alar Cartilages, respecting domes, and Band of Temporal
Fascia.

Figure 6: Type III. Total resection of alar
cartilages, respecting domes. Applicable to noses whose nasal base is very
close to the objective (equilateral nasal base). Band of Temporal Fascia. Used
about 30% of the cases.
3.1.1. Type IV (Figure 7,8)
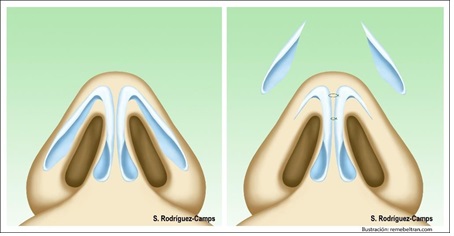
Figure 7: Illustration Type IV. No Temporal Fascia.

Figure 8: Type IV. Total resection of alar
cartilages, respecting domes, and leaving two small alar wedges whose
latero-caudal length is no longer than 8 mm and is of an arrow-tip shape.
Indicated for cases where the nasal base is already equilateral. Used about 35%
of the cases.
3.1.5.
Type V (Figure 9,10)
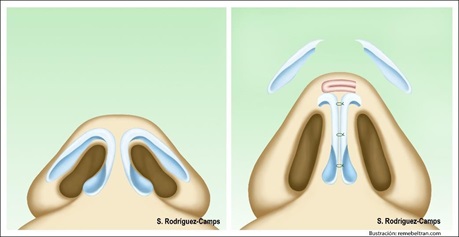
Figure 9: Illustration Type V.
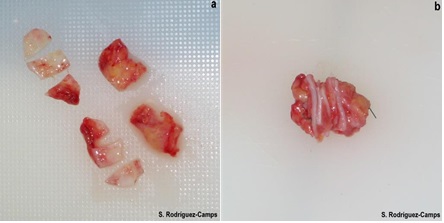

Figure 10: Type V. Total resection of alar cartilages, respecting domes and approaching the Crus Medialis feet, and suturing domes as high as possible to accomplish projection. Then we remove vestibular wedges, place a Converse stitch, smoothly
reduce the soft triangles, release the columella of the base and remove a trunk of
the septum depressor muscle. Generally, it is only here where
we introduce a septum tutor intercrus to prolong and strengthen the columella projecting the nasal tip. This is
indicated for flat, broad, and negroid noses with a short columella, separated nasal wings
and broad nostrils.

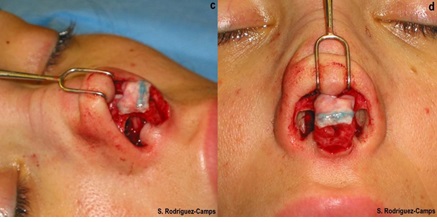
Figure 11: Details of temporal fascia arranged
to be utilized for reconstruction purposes. A fascia seal covering the ends of
the crus medialis in the reconstruction.
4.1.
Type I (Figure 12 a,b)
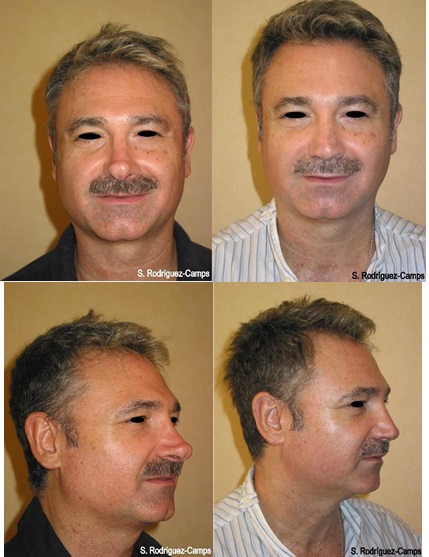
Figure 12a: Type I. Secondary Rhinoplasty. Pacient
operated twice in other centers. Result 1 year later.

Figure 12b: Secondary rhinoplasty. “Pinocchio”
nose. Inadequately removed thick alar cartilages. Treatment was Type I resection-reconstruction.: Total Resection
of the Alar Cartilages, including domes and a trunk of crus medialis. Patch and
band of temporal fascia for covering. Killian septoplasty. Result after 1 year.
4.2 Type II (Figure 13 a,b)


Figure 13b: Secondary Rhinoplasty. Type II resection-reconstruction: Total resection
of the Alar Cartilages, including domes. Patch and band of Temporal Fascia.
Result after 1 year.
Type III (Figure 14 a,b)

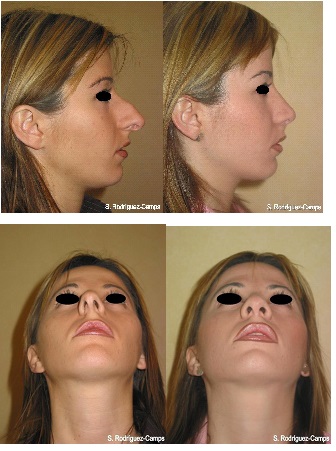
Figure 14b: Primary rhinoplasty. Protruding and bulbous tip with very thick skin. Type III resection-reconstruction:
Total Resection of the Alar Cartilages, respecting domes. There was no need for
temporal fascia given the thickness of the skin.
1
year later.
1.4.
Type IV (Figure 15 a,b)

Figure 15a: Type IV.
Primary Rhinoplasty. Result 1 year later.

Figure 15b: Type IV.
Primary Rhinoplasty. 17 years old patient. 1 year later.
4.5.
Type V (Figure 16 a,b)


Figure 16b: Primary rhinoplasty. Broad tip with a
thick skin and a retracted columella. Type V resection-
reconstruction.Total Resection of the Alar Cartilages, respecting domes and
suturing both crus medialis high. Temporal fascia patch, Intercrus-medialis
tutor and filled in nasal-labial angle. Result after 1 year.
1.
Converse J (1977) Reconstructive Plastic Surgery. (Second Edition), WB
Saunders Company. Philadelphia, London, Toronto 2: 1040-1281.
2.
Goldman IB (1957)
Eye Ear Nose Throat Mon 36: 742-743.
6.
Peck G (1984)
Techniques in Aesthetic Rhinoplasty. (First Edition), Gower Medical Publishing
Ltd. New York, NY, USA.
7.
Sheen J
(1978) Aesthetic Rhinoplasty. (Second Edition), The C.V. Mosby Company. Saint
Louis.
8.
Tardy ME Jr (1990) Surgical Anatomy of the Nose.
(FirstN Edition), Raven Press, Ltd. New York, USA.
10.
Rodríguez-Camps S (1989) Secondary Rhinoplasty in Cleft Nose. Rethi Technique. XX Spanish National Plastic, Reconstructive and
Aesthetic Surgery Society (SECPRE) Meeting. Video Presentation. León, Spain.
11.
Rodríguez-Camps S (1994) Nasal Reconstruction after Mohs
Micrographic Surgery. Poster. Spanish National Reconstructive, Aesthetic and
Plastic Surgery Society (SECPRE) Congress. Valladolid, Spain.
12. Rodríguez-Camps S (1995)
Reconstrucción Nasal tras Cirugía
Micrográfica de Mohs. Cir Plast Iberolatinoamer XXI: 215-223.
13.
Rodríguez-Camps S (1995) Total Reconstructive Rhinoplasty with the medial forehead flap”. VIII Spanish National Reconstructive, Aesthetic
and Plastic Surgery Society (SECPRE) Congress. Video Presentation. Santiago de
Compostela, Spain.
14.
Rodríguez-Camps S (1995) Nose Reconstruction with medial
forehead flap after Mohs Surgery”. International Video-Journal of Plastic and
Aesthetic Surgery 2.
15.
Rodríguez-Camps S (1996) Aesthetic Rhinoplasty under local
anesthesia without sedation”. XXXI Spanish National Reconstructive, Aesthetic and Plastic Surgery Society (SECPRE) Congress. Video Presentation. Madrid, Spain.
16.
Rodríguez-Camps S (1997) Augmentative Rhinoplasty with auricular cartilage. Spanish National Reconstructive, Aesthetic and
Plastic Surgery Society (SECPRE) Congress. Barcelona, Spain
17.
Rodríguez-Camps S (1998) Relapsing Basal Cell Epithelioma of
the nasal tip. Resection. Two-stage reconstruction
with a frontal flap. Nasal Plastic Surgery Symposium, tribute to Dr.
Vilar-Sancho. The Ramón y Cajal Hospital, Madrid, Spain.
19.
Rodriguez-Camps
S (1999) Miscellaneous Rhinoplasty: Primary and Secondary. XXXIV Spanish
National Reconstructive, Aesthetic and Plastic Surgery Society (SECPRE)
Congress. Marbella, Spain.
20.
Rodríguez-Camps S (2000) Rhinoplasty: Primary, Secondary
and Reconstructive. II Plastic, Reconstructive and Aesthetic Surgery Society
Meeting of the Valencian Community (SCPRECV). Alicante, Spain.
21.
Rodríguez-Camps
S (2001) Nasal Reconstruction After Epithelioma. Aesth Plastic Surg 25:
273-277.
22.
Rodríguez-Camps S (2002) Aesthetic Nasal Reconstruction.
from the Oficial Book of the XXXVII Spanish National Reconstructive, Aesthetic and Plastic Surgery Society (SECPRE) Congress. Rhinoplasty,
Spain.
23.
Rodríguez-Camps S (2004) Rhinoplasty. The Aesthetic
Tip-Columella-Lip Unit. XV Latin American
Federation of Plastic Surgery Congress (FILACP) and XXXIX Spanish National
Reconstructive, Aesthetic and Plastic Surgery Society (SECPRE) Congress.
Seville, Spain.
24.
Rodríguez-Camps S (2004) Rhinoplasty: Nasal Base. V
Plastic, Reconstructive and Aesthetic Surgery Society Meeting of the Valencian
Community (SCPRECV). General University Hospital, Alicante, Spain.
25.
Rodríguez-Camps S (2005) Nasal Reconstruction. VI National
Reconstructive, Aesthetic and Plastic Surgery Society Meeting of the Valencian
Community (SCPRECV). Valencia, Spain.
26.
Rodríguez-Camps S (2005) Closed Rhinoplasty. Teaching
Course on National Reconstructive, Aesthetic and Plastic Surgery. School of
Medicine. University of Barcelona, Spain.
27.
Rodriguez-Camps
S (2006) Secondary Rhinoplasty: Our procedure. Total Resection of the Alar
Cartilages and Domes with a Temporal Fascia Stamp on the Tip. XLI Spanish
National Reconstructive, Aesthetic and Plastic Surgery Society (SECPRE)
Congress. Paper. Pamplona, Spain.
28.
Rodríguez-Camps S (2006) Nasal Reconstruction. VII
Reconstructive, Aesthetic and Plastic Society Meeting of the Valencian
Community (SCPRECV) Meeting. Alzira, Valencia, Spain.
29.
Rodríguez-Camps S (2006) Reconstructive Rhinoplasty. Teaching Course on Reconstructive, Aesthetic and Plastic
Surgery. School of Medicine. University of Barcelona, Spain.
30.
Rodríguez-Camps S (2008) Rhinoplasty. The Difficult Nasal
Tip: Total Resection of the Alar Cartilages”. XIX Congress of the International
Society of Aesthetic Plastic Surgery, (ISAPS). Panelist. Melbourne, Australia.
33.
Rodríguez-Camps S (2010) New technique to treat a very
difficult nasal tip. Total resection of the Alar Cartilages and
Temporal Fascia Covering. XLV Spanish National Reconstructive, Aesthetic and
Plastic Surgery Society (SECPRE) Congress. Gerona, Spain.
34.
Rodríguez-Camps S (2010) Demonstrating the Total Resection of the Alar Cartilages and
Temporal Fascia Technique on a corpse as part of the VI Theoretical-Practical
Course on Anatomical Dissection
organized by the Spanish Association of Aesthetic Plastic Surgery (AECEP). I
Course on Rhinoplasty and Facial Implants”. Department of Human Anatomy and
Embryology II, School of Medicine at the Complutense University of Madrid.
Madrid, Spain.
35. Rodríguez-Camps S (2010) Un paso adelante en Rinoplastia: Técnica
de Resección Total
de los Cartílagos Alares y
Fascia Temporal. Spanish
Association of Aesthetic Plastic Surgery Journal (AECEP) 12: 13-24.
36.
Rodríguez-Camps S (2011) Rhinoplasty. The Difficult Nasal
Tip. Total Resection of the Alar Cartilages and Temporal Fascia Technique. A 24 Year Experience. In: Brenner MJ, (ed.). Rhinoplasty. Rijeka, Croatia: Intech. Pg No: 97-114.
37.
Rodríguez-Camps S (2013) Personal treatment of the
Projection Disorders: very projected and very few projected Tip. XLVIII National Congress of the Spanish Society of Plastic, Reconstructive and Aesthetic Surgery (SECPRE).
Tenerife.
38.
Rodríguez-Camps S (2013) First Kuwait Aesthetic Surgery
Conference. The Difficult Nasal Tip. Total Resection of the Alar Cartilages and
Temporal Fascia Technique. Guest Professor. Kuwait City.
39.
Rodríguez-Camps S (2015) Total Resection of the Alar
Cartilages and Temporal Fascia Technique in Rhinoplasty. In: Di GiuseppeA, Shiffman M, (ed.). New Frontiers in Plastic and Cosmetic Surgery. New Delhi, India Pg
No:77-94.
40.
Rodríguez-Camps S (2016) A
New Technique in Rhinoplasty. Day of Residents. Update in Facial Aesthetic Surgery. Guest Professor. Spanish Society of
Plastic, Reconstructive and Aesthetic Surgery (SECPRE).
Illustrious College
of physicians of Madrid.
41.
Rodríguez-Camps S (2016) I Rhinoplasty Course, organized by
the Spanish Society of Plastic, Reconstructive and Aesthetic Surgery (SECPRE).
Teacher. Course Director. Central Operating Theaters of the Casa de Salud University Hospital in Valencia.
42.
Rodríguez-Camps S (2017) II Rhinoplasty Course, organized by
the Spanish Society of Plastic, Reconstructive and Aesthetic Surgery (SECPRE).
Teacher. Course Director. Central Operating Theaters of
the Casa de Salud University Hospital in Valencia.
43.
Rodríguez-Camps S (2017) Some Less Usual, or Never Used,
Technical Resources in Rhinoplasty for Nasal Base Improvement. Clinics in
Surgery Journal Pg No:1529.
44.
Rodríguez-Camps S (2017) III
Rhinoplasty Course, organized by the Spanish Society of Plastic,
Reconstructive and Aesthetic Surgery (SECPRE). Teacher. Course Director.
Central Operating Theaters of the Casa de Salud
University Hospital in Valencia.
45.
Rodríguez-Camps S (2017) II International Congress AECEP
Meeting 2017. "Leporine Septorhinoplasty. Personal Technique: Total
Resection of the Alar Cartilages and Temporal Fascia (T.R.T.C.A. + F.T.), TYPE
III". Video- Conference. Fine Arts Circle, Madrid.
46.
Rodríguez-Camps S (2017) Septorhinoplasty with Septum Perforation in Cocaine Patient Overcome her Addiction. European Aesthetic
Plastic Surgery Journal (AECEP) 7: 39-43.
47.
Rodríguez-Camps S (2016) Doctoral Thesis: Excellent Cum Laude. A new Technique of Nasal tip Reshaping
in Rhinoplasty, for Extremely Difficult Cases, by the Total Resection of the
Alar Cartilages and Temporal Fascia. Surgery Department of the Faculty of
Medicine and Odontology at the University of Valencia. University of Valencia.
48.
Burget G,
Menick F (1994) Aesthetic Reconstruction of the Nose. (First Edition), Mosby.